
 By Drew Ivan, Chief Product and Strategy Officer, Lyniate
By Drew Ivan, Chief Product and Strategy Officer, Lyniate
Twitter: @lyniate
The use of telehealth has grown exponentially since the spread of Covid-19. With the surge of virtual visits, it’s crucial that health IT vendors creating telehealth solutions — as well as providers who are adding telehealth platforms to their practices — ensure their IT infrastructure is set up to handle new data flows.
Proper data flows in a telehealth environment impact not only continuity of patient care, but also revenue generation. This is where interoperability among different systems — the provider’s EMR or practice management system, scheduling system, and billing system — comes into play.
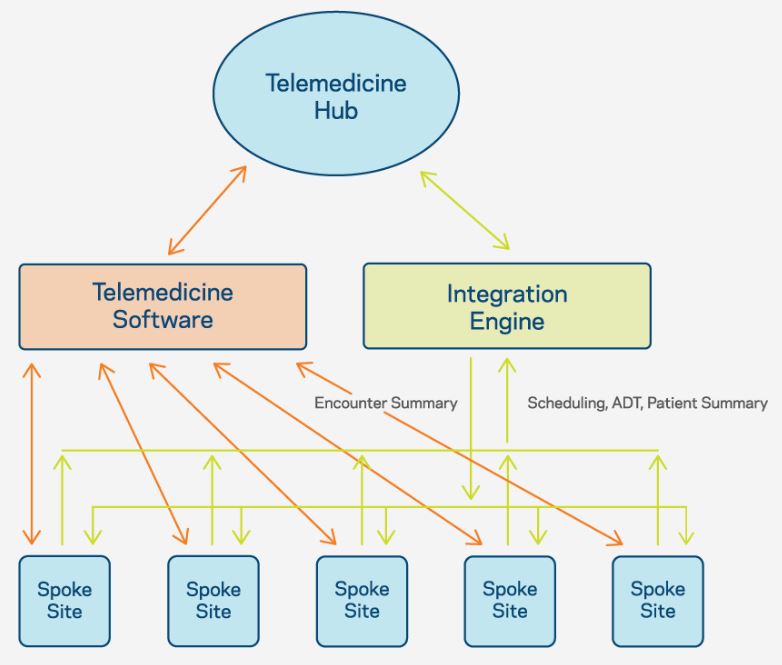
The typical telehealth hub-and-spoke model has started to prove its value to healthcare, but as the platforms become more ingrained within organizations and the business of healthcare evolves, new needs are arising that center on interoperability and how to unlock essential information.
For a heterogeneous health system using telemedicine to extend the reach of its specialists the hub location (e.g. centralized hospital), the spoke site (e.g. a community clinic), and patients already have a relationship. Typically, this means everyone is connected via the same EHR; doctors at the hub site are on the same system as the spoke site, and the patient’s charts and appointments are already in the system.
However, a growing trend in telemedicine is for best-in-class hospitals to provide their specialist services to their affiliated hospital network and to other more loosely tied customers — which can be a double-edged sword.
While this does offer new services with a greater reach, the hub and spoke will not have the same EHR system, and clinicians at the hub will not have access to patient data at the spoke — locking critical information away from the clinicians who need it.
In these increasingly common implementations, the only solution is rich interoperability among those systems:
- The hub EHR
- The multiple spoke EHRs
- The telehealth platform itself
With this scenario, the biggest issue for clinicians relates to workflow. How can a scheduler at a spoke create an appointment for a clinician at the hub? How can the hub clinician see a schedule comprised of appointments across all spokes on one screen? And how can they review patient records prior to each appointment?
The solution relies on orchestrated workflow across several institutions’ systems to send and receive patient scheduling messages (usually HL7 v2.x SIU messages) and exchange patient summary documents (often CCD or C-CDA format).
Data flow can also be an issue. In situations where a hub clinician is treating a spoke patient, they may document the encounter in the hub institution’s EHR. Or, the workflow may require the encounter to be documented in the telemedicine software itself. In either case, a copy of the encounter note will need to be transferred to the spoke institution’s EHR system (common formats for this include: CCD, C-CDA, MDM, ORU, or a simple PDF file).
Today, it’s impossible to treat interoperability as a feature of telemedicine software or as a step in a telemedicine implementation project. A robust data exchange strategy needs to be the foundation of an institution’s telemedicine approach to unlock data and make it a success for providers, clinicians, and their patients.
This article was originally published on the Lyniate blog and is republished here with permission.